Overview

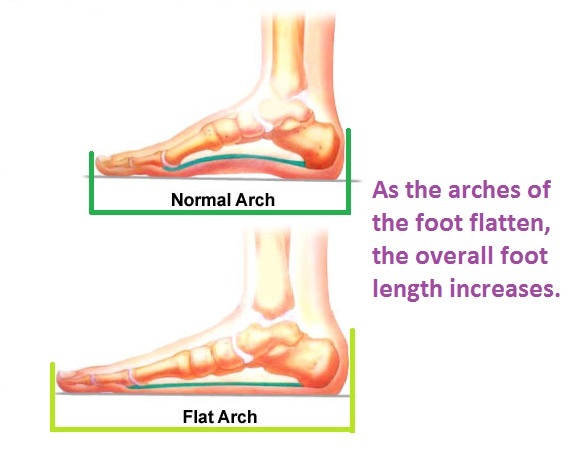
In a normal foot, the tendons in your foot and lower leg work together to form the arch. When the tendons all pull properly, your foot forms a moderate, normal arch. When the tendons do not pull together properly, there is little or no arch, called flat foot or fallen arch. Children are born with flat feet. In infants and toddlers, prior to walking, the longitudinal arch is not developed and flat feet are normal. As children begin standing on their toes, the muscles start to develop and an arch appears. The arch continues to develop throughout childhood, and by adulthood most people have developed normal arches. But in some cases the arch doesn?t form completely.
Causes
Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with a nerve problem that limits normal feeling in the feet, can have arch collapse. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. This is because patients do not feel pain as the arch collapses. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate, without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Podiatrists are trained in expertly assessing flat feet and identifying different risk factors and the causes for it. Initial assessment will begin with a detailed history attempting to find out if any underlying illness has resulted in this. A detailed clinical examination normally follows. The patient may be asked to perform certain movements such as walking or standing on their toes to assess the function of the foot. Footwear will also be analysed to see if there has been excessive wear or if they are contributing to the pronation of the foot. To assess the structure of the foot further, the podiatrist may perform certain x-rays to get a detailed idea of the way the bones are arranged and how the muscle tissues may be affecting them. It also helps assess any potential birth defects in a bit more detail.
arch supports for high arches
Non Surgical Treatment
The simplest form of treatment is the use of custom fitted orthotics. For this, it is best to see a podiatrist, who is a trained medical professional that assesses feet and gives you a prescription for the orthotic. If the orthotics do not work - or if the deformity is very severe - then surgical management may be needed. There is a very wide range of procedures available, with varying downtimes and complexity. The simplest procedure of all is a simple calf release. This can be done at the back of the knee or the calf, and has a very quick recovery. It is a day-surgery procedure, and the patient can walk immediately after the surgery without the need for a cast. Recovery back to jogging can be as early as three weeks. The calf release stops the deforming force but obviously does not correct the arch itself. It is usually done in combination with some of the other procedures mentioned below. Done by itself, the patient will probably still require orthotics but by releasing the calf, it allows the orthotics to be much more effective. The other end of the spectrum is a complete reconstruction of the arch with bone work and screws to fuse joints.
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
In a normal foot, the tendons in your foot and lower leg work together to form the arch. When the tendons all pull properly, your foot forms a moderate, normal arch. When the tendons do not pull together properly, there is little or no arch, called flat foot or fallen arch. Children are born with flat feet. In infants and toddlers, prior to walking, the longitudinal arch is not developed and flat feet are normal. As children begin standing on their toes, the muscles start to develop and an arch appears. The arch continues to develop throughout childhood, and by adulthood most people have developed normal arches. But in some cases the arch doesn?t form completely.
Causes
Inflammatory arthritis, such as rheumatoid arthritis, can cause a painful flatfoot. This type of arthritis attacks not only the cartilage in the joints, but also the ligaments that support the foot. Inflammatory arthritis not only causes pain, but also causes the foot to change shape and become flat. The arthritis can affect the back of the foot or the middle of foot, both of which can result in a fallen arch. An injury to the ligaments in the foot can cause the joints to fall out of alignment. The ligaments support the bones and prevent them from moving. If the ligaments are torn, the foot will become flat and painful. This more commonly occurs in the middle of the foot (Lisfranc injury), but can also occur in the back of the foot. In addition to ligament injuries, fractures and dislocations of the bones in the midfoot can also lead to a flatfoot deformity. People with diabetes or with a nerve problem that limits normal feeling in the feet, can have arch collapse. This type of arch collapse is typically more severe than that seen in patients with normal feeling in their feet. This is because patients do not feel pain as the arch collapses. In addition to the ligaments not holding the bones in place, the bones themselves can sometimes fracture and disintegrate, without the patient feeling any pain. This may result in a severely deformed foot that is very challenging to correct with surgery. Special shoes or braces are the best method for dealing with this problem.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. The symptoms of PTTD may include pain, swelling, a flattening of the arch, and an inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, when PTTD initially develops, there is pain on the inside of the foot and ankle (along the course of the tendon). In addition, the area may be red, warm, and swollen. Later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle.
Diagnosis
Podiatrists are trained in expertly assessing flat feet and identifying different risk factors and the causes for it. Initial assessment will begin with a detailed history attempting to find out if any underlying illness has resulted in this. A detailed clinical examination normally follows. The patient may be asked to perform certain movements such as walking or standing on their toes to assess the function of the foot. Footwear will also be analysed to see if there has been excessive wear or if they are contributing to the pronation of the foot. To assess the structure of the foot further, the podiatrist may perform certain x-rays to get a detailed idea of the way the bones are arranged and how the muscle tissues may be affecting them. It also helps assess any potential birth defects in a bit more detail.
arch supports for high arches
Non Surgical Treatment
The simplest form of treatment is the use of custom fitted orthotics. For this, it is best to see a podiatrist, who is a trained medical professional that assesses feet and gives you a prescription for the orthotic. If the orthotics do not work - or if the deformity is very severe - then surgical management may be needed. There is a very wide range of procedures available, with varying downtimes and complexity. The simplest procedure of all is a simple calf release. This can be done at the back of the knee or the calf, and has a very quick recovery. It is a day-surgery procedure, and the patient can walk immediately after the surgery without the need for a cast. Recovery back to jogging can be as early as three weeks. The calf release stops the deforming force but obviously does not correct the arch itself. It is usually done in combination with some of the other procedures mentioned below. Done by itself, the patient will probably still require orthotics but by releasing the calf, it allows the orthotics to be much more effective. The other end of the spectrum is a complete reconstruction of the arch with bone work and screws to fuse joints.
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Stage one deformities usually respond to conservative or non-surgical therapy such as anti-inflammatory medication, casting, functional orthotics or a foot ankle orthosis called a Richie Brace. If these modalities are unsuccessful surgery is warranted. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss. Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.



 A Morton's neuroma, or interdigital neuroma, is a painful condition which involves a nerve on the plantar aspect (bottom) of the foot. Occasionally a neuroma develops following a bruising injury to the sole of the foot, such as might be caused by jumping onto a rock or other objects, but in general, the origin of the condition is unknown.
A Morton's neuroma, or interdigital neuroma, is a painful condition which involves a nerve on the plantar aspect (bottom) of the foot. Occasionally a neuroma develops following a bruising injury to the sole of the foot, such as might be caused by jumping onto a rock or other objects, but in general, the origin of the condition is unknown.






 Overview
Overview Symptoms
Symptoms A bunion is a firm, fluid-filled pad overlying the inside of the joint at the base of the big toe (metatarsophalangeal joint). The pad (bursa), which may get larger and stick out, can become inflamed and painful. Bunions may run in families, but many result from wearing tight shoes. Nine out of 10 bunions are developed by women. Nine out of 10 women wear shoes that are too small. Tight shoes also can cause other disabling foot problems like corns, calluses and hammertoes.
A bunion is a firm, fluid-filled pad overlying the inside of the joint at the base of the big toe (metatarsophalangeal joint). The pad (bursa), which may get larger and stick out, can become inflamed and painful. Bunions may run in families, but many result from wearing tight shoes. Nine out of 10 bunions are developed by women. Nine out of 10 women wear shoes that are too small. Tight shoes also can cause other disabling foot problems like corns, calluses and hammertoes.
